Body Composition Profiling: The precise way to measure
Your patients are relying on you to make optimal diagnostic and treatment decisions, however, your tools remain imprecise—leaving you to fill in critical gaps when making go/no-go treatment decisions. You need a new standard in body composition analysis that will provide precise patient insights.
Is BCP available in your region?
AMRA® BCP Scan
The AMRA® BCP Scan is a neck-to-knee MRI-based service using our validated protocols for creating an individualized Body Composition Profile (BCP). After we analyze the images, you receive an easy-to-interpret report containing precise body composition measurements with comparison to normative values.
- Evaluate the distribution of abdominal fat into visceral fat and subcutaneous fat
- Assess the health and volume of specific muscle groups
- Encourage your patients by visualizing small and large body composition changes over time that are not outwardly visible
- Save time and resources by expanding the value of an already-prescribed MRI by simply adding the BCP scan protocol—no need for an additional appointment.
Why BCP?
Lifestyle choices and several diseases affect body fat and muscles. These changes are detectable when the precision of the fat and muscle measurements is sufficiently high to assess, for example, longitudinal changes and treatment results. This is what the AMRA® BCP Scan was built for—offering precise measurements.
Applications of BCP Scan:

Weight Loss Management
BCP Scan provides information to support weight loss management, measuring the volume of visceral fat, subcutaneous fat, and thigh muscles in relation to a reference population. It also measures the fat fraction in the liver and thigh muscles.
Literature has shown that weight loss by GLP-1 agonist treatment as well as bariatric surgery leads to a reduction in weight, visceral fat, subcutaneous fat, and liver fat 2,6,12,5. Furthermore, muscle volume is strongly related to body size, and losing weight by GLP-1 treatment, diet, exercise, and bariatric surgery may also lead to muscle loss 3,6,8,12. Importantly, the response to weight loss managing strategies on an individual level is heterogenic 4.
Fat distribution impact
BCP Scan can be used to identify individual visceral fat and liver fat distribution patterns. Literature has shown that certain distribution patterns with high visceral fat are linked to incident heart disease as well as new-onset type 2 diabetes and that loss of visceral fat among individuals with excess visceral fat is associated with cardiometabolic benefits 11,15,7. This scientific literature supports physicians in identifying individuals with cardiometabolic high-risk fat distribution patterns during weight loss management.
Muscle health impact
BCP Scan can be used to identify individuals with lower-than-expected muscle volume and elevated muscle fat content. Literature has shown that low muscle volume with high muscle fat content is predictive of mortality, linked to poor functional performance, and that muscle loss occurs during weight loss interventions 3,6,8,9,12. This information supports physicians in understanding muscle health during weight loss management.

Longevity
Biomarkers describing muscle health
Monitor the impact of your exercise and rehabilitation guidance on muscle volume (quantity) and muscle fat (quality) as measured by BCP Scan. Literature has shown that low muscle volume and high muscle fat are associated with poor functional performance and that exercise may lead to increased muscle volume and reduction in muscle fat in healthy individuals 13,8,10. This may help your patients understand if their exercise program is working or if it needs more optimization. In addition, normal aging and inactivity cause 3% to 5% muscle loss each decade after age 30 16. Incorporating the BCP Scan into a longevity plan to help individuals assess their health and wellness over time could help optimize their body composition measurements. Periodically measuring fat and muscle volume to support an active lifestyle well into their senior years can also support these goals.

Preventative Health
Biomarkers linked to incident heart disease
BCP Scan can identify individuals with high visceral fat and low liver fat. Literature has shown that this phenotype is associated with a high risk of incident heart disease 15,7. Exercise, diet, pharmacological treatment, and surgical interventions are associated with a reduction in visceral fat and loss of visceral fat is associated with cardiometabolic benefits among individuals with excess visceral adiposity 12,5,11. This fact supports physicians in identifying patients with a high risk of incident heart disease and measuring treatment impact on visceral adiposity.
Biomarkers linked to new onset type 2 diabetes
BCP Scan measures visceral fat volume and liver fat fraction. Elevated visceral fat and liver fat have been shown in literature to be strong risk factors of new-onset type 2 diabetes 15,7. This scientific literature supports physicians in identifying patients with an elevated risk of new-onset type 2 diabetes. Visceral fat and liver fat can be reduced, and the reduction of visceral fat is associated with cardiometabolic benefits 11.
Biomarkers supporting diagnosis of liver steatosis
BCP Scan measures liver proton density fat fraction (PDFF). Clinical practice guidelines recognize MRI PDFF as the most accurate non-invasive method for diagnosing and quantifying liver steatosis 14,1.
Effortless & Cloud-Based Digital Health
1. Getting Started

Setup & Verification using
AMRA® Protocol
2. Scanning
Rapid MRI
3. Data Transfer
Safe & Secure Image Transfer
4. Analysis
Automated Segmentation, Quantification & QA
5. Delivery

Body Composition
Report

Key Features
High Accuracy, High Precision
Through automated image calibration and segmentation, as well as reliable fat and muscle quantification, our results are accurate and precise.
Rapid, Neck-to-knee MRI
Image multiple areas of the body within a single scan, send those images to us for analysis, and get muscle and fat measurements with comparison to normal ranges.
Patient-Friendly
Establish the best-possible MRI patient experience, and keep your clinical workflows moving with a quick, simple, and radiation-free MRI scan.
Easy-to-Interpret
With our report, you’ll easily understand your patient’s body composition profile to make optimal decisions promptly.
Rapid Turnaround
Get your imaging results quickly! With our team of experts and automated analysis and quantification, you get results fast.
Quality-Controlled
With a robust QC program, our reference database and patient datasets are accurate and precise. Our solutions are regulatory compliant, with detailed documentation and audit trails.
Easy Integration & No Installation
BCP Scan integrates easily with imaging protocols and technologies and is standardized across major 1.5 T and 3 T MR scanners.
Secure Data Transfer
Our security measures ensure your data is transferred safely and smoothly using our cloud-based solutions.
What you receive
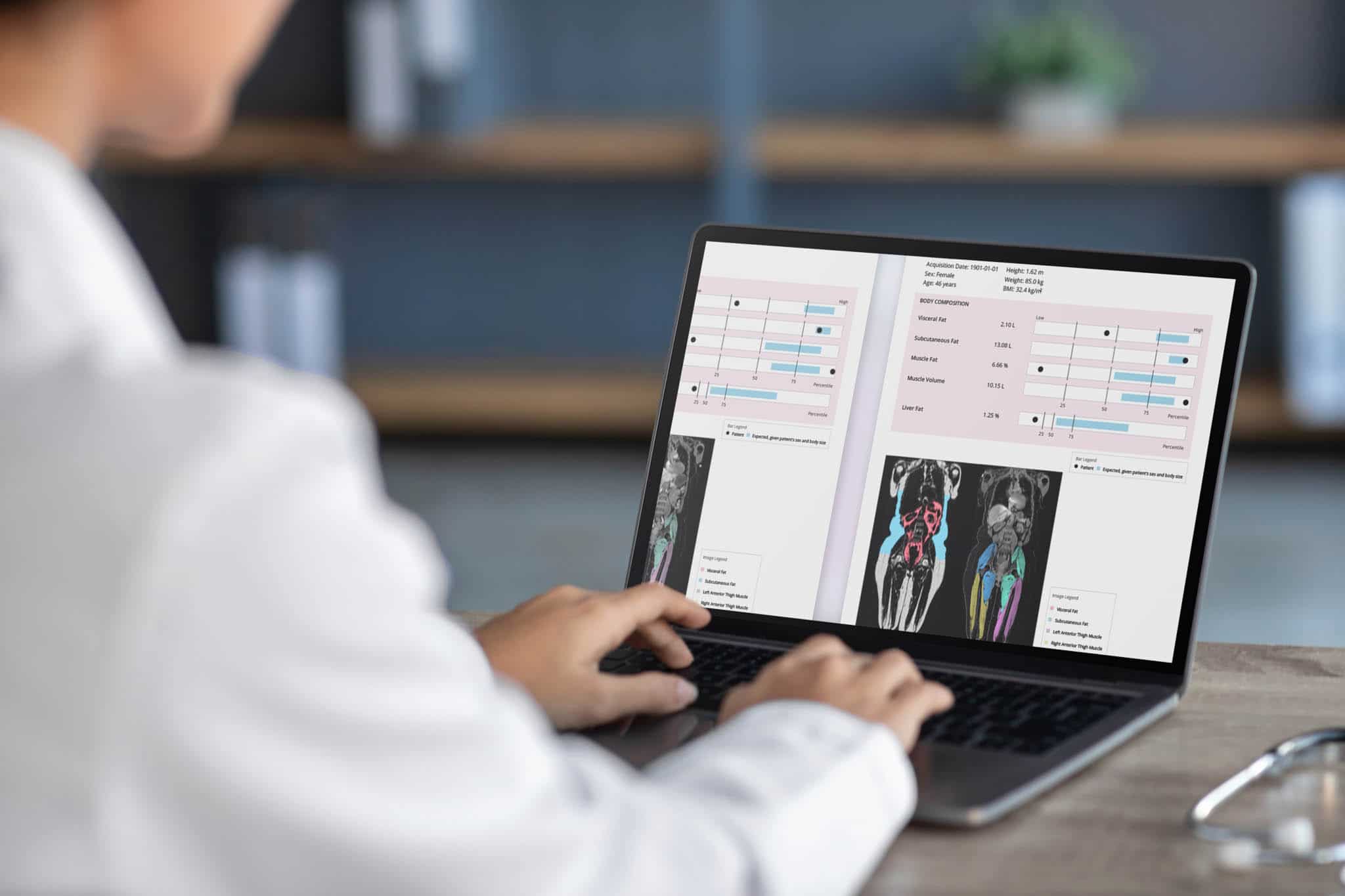
AMRA® BCP Scan Report
It’s meaningful, actionable, and concise
Our measurements are delivered in the form of an individualized report where your patient’s measurements are compared to normal ranges based on our reference database. To ensure our comparisons are relevant to your patient, each individual is compared to control groups with similar characteristics such as sex and BMI.
Body composition measurements
- Visceral Fat
- Subcutaneous Fat
- Muscle Fat
- Muscle Volume
- Liver Fat

From Body Mass Index to Body Composition Profiling: A slim body is not always equal to a healthy body
Investigational Studies for Future Use
Clinical Effectiveness of Body Fat Distribution Imaging in Real-World Practice: The BODY-REAL Study (BODY-REAL)
The goal is to determine the real-world feasibility and utility of body fat imaging using rapid MRI to enhance risk perception, induce behavioral change, and improve clinical outcomes in overweight and obese individuals.

Get Precise Body Composition Measurements with AMRA
When you partner with AMRA for your clinical MRI needs, you benefit from our unrivalled digital health platform and normative database for body composition analysis—generated by our team of analysis engineers and body composition researchers.
You and your patients are at the top of our priority list when we design our MRI-based technology and services. Our vast experience in body composition analysis and constant-improvement mentality equips our team with the skills, knowledge, and passion required to develop the solutions you need.
How We Do It
Get a glimpse of how we use our digital health platform to generate and evolve our technologies and biomarkers.
Why It Matters
Understand why a new standard in body composition analysis is needed and how it can improve the lives of clinicians and their patients.
Our Core Areas
Explore our areas of focus—ranging from health and wellness to common metabolic diseases to rare neuromuscular diseases.
References
1.Berzigotti A, Tsochatzis E, Boursier J, Castera L, Cazzagon N, Friedrich-Rust M, et al. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis—2021 update. J Hepatol. 2021;75:659–89. https://doi.org/10.1016/j.jhep.2021.05.025
2. Covarrubias Y, Fowler KJ, Mamidipalli A, Hamilton G, Wolfson T, Dahlqvist Leinhard O, et al. Pilot Study on longitudinal change on pancreatic proton density fat fraction during a weight-loss surgery program in adults with obesity. J Magn Reson Imaging 2019; 50(4):1092-1102. https://dx.doi.org/10.1002/jmri.26671
3. Chaston TB, Dixon JB, and O’Brien PE. Changes in fat-free mass during significant weight loss: a systematic review. International Journal of Obesity. 2007: 31;743-750. https://dx.doi.org/10.1038/sj.ijo.0803483
4. Dent R, McPherson R, and Harper ME. Factors affecting weight loss variability in obesity. Metabolism 2020:113;154388. https://doi.org/10.1016/j.metabol.2020.154388
5. Gastaldeli A, Cusi K, Fernández Landó L, Bray R, Brouwers B, and Rodríguez Á. Effect of tirzepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI): a substudy of the randomised, open-label, parallel-group, phase 3 SURPASS-3 trial. Lancet Diabetes & Endocrinology. 2022; 10(6):393-406. https://doi.org/10.1016/S2213-8587(22)00070-5
6. Kengott HG, Nickel F, Wise PA, Wagnet F, Billeter AT, Nattenmüller J, et al. Weight loss and changes in adipose tissue and skeletal muscle volume after laparoscopic sleeve gastrectomy and roux-en-y gastric bypass: A prospective study with 12-month follow-up. Obesity Surgery. 2019: 29;4018-1028. https://doi.org/10.1007/s11695-019-04087-w
7. Linge J, Cariou B, Neeland IJ, Petersson M, Rodríguez Á, et al. Skewness in body fat distribution pattern links to specific cardiometabolic disease risk profiles. The Journal of Clinical Endocrinology & Metabolism. 2023 dgad570. https://doi.org/10.1210/clinem/dgad570
8. Linge J, Heymsfield SB, and Dahlqvist Leinhard O. On the definition of sarcopenia in the presence of aging and obesity – Initial results from the UK Biobank. J Gerontol A Biol Sci Med Sci. 2020; 75(7):1309-1316. https://dx.doi.org/10.1093/gerona/glz229
9. Linge J, Petersson M, Forsgren MF, Sanyal AJ, and Dahqlvist Leinhard O. Adverse muscle composition predicts all-cause mortality in the UK Biobank imaging study. Journal of Cachexia, Sarcopenia and Muscle. 2021; 12:0513-1526. https://dx.doi.org/10.1002/jcsm.12834
10. Linge J, Ekstedt M, and Dahlqvist Leinhard. Adverse muscle composition is linked to poor functional performance and metabolic comorbidities in NAFLD. JHEP Reports. 2021: 3(1);100197. https://doi.org/10.1016/j.jhepr.2020.100197
11. Neeland IJ, Ross R, Deprés JP, Matsuzawa Y, Yamashita S, Shai I, et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: a position statement. Lancet Diabetes & Endocrinology. 2019; 7(9):715-725. http://dx.doi.org/10.1016/S2213-8587(19)30084-1
12. Neeland J, Marso SP, Ayers CR, Lewis, B, Oslica R, et al. Effects of liraglutide on visceral and ectopic fat in adults with overweight and obesity at high cardiovascular risk: a randomised, double-blind, placebo-controlled, clinical trial. Lancet Diabetes & Endocrinology. 2021; 9(9):595-605. https://doi.org/10.1016/S2213-8587(21)00179-0
13. Mandic M, Rullman E, Widholm P, Lilja M, Dahlqvist Leinhard O, Gustafsson T, et al. Automated assessment of regional muscle volume and hypertrophy using MRI. Scientific Reports. 2020;10:2239. https://doi.org/10.1038/s41598-020-59267-x
14. Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, Abdelmalek MF, Caldwell S, Barb D, et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023;77:1797–835. https://doi.org/10.1097/hep.0000000000000323
15. Tejani S, McCoy C, Ayers CR, Powel-Wiley TM, Després JM, Linge J, et al. Cardiometabolic health outcomes associated with discordant visceral and liver fat phenotypes: Insights from the Dallas Heart Study and UK Biobank. Mayo Clinical Proceedings. 2022;97(2):225-237. https://doi.org/10.1016/j.mayocp.2021.08.021
16. Volpi E, Nazemi R, Fujita S, Muscle tissue changes with aging, Clinical Nutrition and Metabolic Care, 2004Jul;7(4):405-10.https://doi.org/10.1097/01.mco.0000134362.76653.b2

How can AMRA support you and your clients?
Send us a message and we will happily provide more information or a quotation.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.