
AMRA® Body Fat Z-Scores
Revealing the true impact of drug therapies for metabolic diseases through weight-invariant fat distribution assessment using AMRA’s Z-Scores
As the rise of incretin-based therapies has changed the face of type 2 diabetes (T2D) and obesity care, the treatment development landscape has rapidly followed suit and is influencing our perspective on obesity and metabolic disease.
Achieving significant weight reduction is no longer an unobtainable target, and the need for clinically relevant descriptions of adiposity is imminent. Research teams must characterize changes beyond weight loss to reveal the true effect of drugs in development and detangle the large heterogeneity of metabolic disease so that each patient can be treated the right way for them.
Very similiar with
indirect biomarkers
BMI (kg/m2)
Age
A
35.6
37
B
35.4
35
C
35.6
59
D
36.2
49
E
35.8
47
F
35.7
57
Vastly different
with direct body
composition
biomarkers
Liver PDFF (%)
Visceral fat (L)
Subcutaneous fat (L)
Muscle fat infiltration (%)

1.3
1.1
13.5
5.9

4.7
2.1
15.9
8.9

2.6
3.2
12.5
11.4

6.8
8.0
14.0
7.9

0.8
4.7
16.2
10.8
16.8
6.2
16.1
12.0
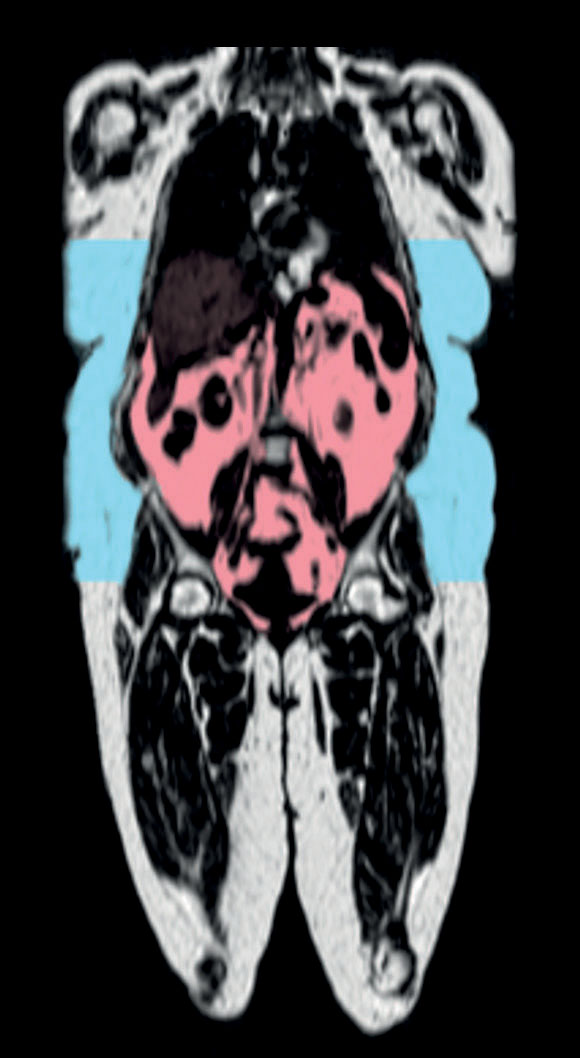
Credit: Collaboration with Dr. Ian J Neeland, University Hospitals Cleveland Data from NCT03038620 analyzed with AMRA® Researcher






Figure 1. Heterogeneity in fat distribution pattern: Six patients enrolled in the same interventional clinical trial evaluating the effect of liraglutide combined with a lifestyle intervention for the treatment of overweight and obesity.
Although the link of Body Mass Index (BMI) to morbidity and mortality is firmly established at the population level, there is significant variability in cardiometabolic risk profile among people with the same BMI. Over the past 30 years, findings from epidemiological studies have shown that visceral adipose tissue (VAT) is an independent risk marker for cardiovascular and metabolic morbidity and mortality. The widened use of magnetic resonance imaging (MRI) has uncovered different patterns of how fat is stored (e.g., as visceral, subcutaneous, or within the liver), possibly providing an explanation for the considerable variability in cardiometabolic risk seen in obesity and across related indications1.
Therefore, targeting reduction of ectopic fat and achieving a balance in fat distribution patterns are highly attractive targets for drug manufacturers aiming to develop therapies with broader metabolic benefits beyond (or instead of) weight reduction. However, with significant weight reductions, people commonly lose all kinds of fat to some extent and, consequently, the race for ectopic fat reduction may become the race towards the largest weight reduction.
As the rapidly rising interest in more clinically relevant descriptions of adiposity (including fat distribution and ectopic fat deposition) mounts alongside the scientific evidence describing its importance, more and more studies are incorporating MRI, encompassing small Phase I, multi-site Phase III, and large outcome trials. As the field is widening through an ever-broadened range of molecules and combination therapies, time is of the essence, and the need for rapid patient recruitment is unprecedented. This new landscape calls for standardized processes and validated biomarkers that enable the use of MRI for endpoints in large multi-site clinical trials, which span over thousands of patients and sites covering a wide range of scanners and field strengths.
To address these challenges, AMRA has developed weight-invariant body fat Z-Scores, based on highly reproducible volumetric measurements of VAT, abdominal subcutaneous adipose tissue (aSAT), and liver fat (proton density fat fraction [PDFF]) derived from carefully calibrated images collected using rapid (8–10 minutes) and standardized image acquisition protocols.2
In order to reveal the true impact of therapies on ectopic fat and to enable differentiation between treatments that achieve varying degrees of weight reduction, clinical trial endpoints capturing changes in ectopic fat independent of body weight are necessary.
The Z-Scores were created in the pursuit of developing biomarkers that move the field closer to understanding whether certain treatments could:
- Possess targeted effects on specific (or several) fat depots (identifying impact beyond weight change)
- Cause shifts in fat distribution patterns (able to change patient phenotype).
The Z-Scores were specifically designed to provide a sex-, height-, weight-, and BMI-invariant assessment by estimating the degree to which each study participant deviates from the average value among matched controls. The reference data is based on more than 55,000 participants included in the UK Biobank imaging study, which since 2015 has used AMRA’s image acquisition protocol for collection of MRI body images, providing reference data with every clinical trial using AMRA® Researcher for body composition analysis.
Cardiometabolic Risk Profiles & Evaluation of Anti-Obesity Treatment
Here, we present:
- Highlights from the first studies that uncover the links between fat distribution patterns and cardiometabolic risk profiles,
- Recent results from pharmacological clinical trials utilizing AMRA® Researcher to evaluate the effects of incretin-based treatments liraglutide, tirzepatide, and retatrutide, and
- Findings from studies using body fat Z-scores for risk stratification in obesity and identification of potential targeted effects on VAT and liver fat from tirzepatide treatment.
1. Discordant visceral and liver fat phenotypes and links to cardiometabolic
health outcomes
The first study investigating fat distribution patterns was conducted using data from the UK Biobank imaging study. Back in 2018, 6,000 participants were imaged and had completed body composition analysis with AMRA® Researcher. As the observation time was short, a cross-sectional study was performed describing the fat distribution pattern of participants without any metabolic diseases, as well as participants with T2D and cardiovascular disease (CVD)3. In line with findings from previous studies, the results showed VAT was strongly associated with both CVD and T2D, while there was no significant association with aSAT for any of the diseases when taking the magnitude of VAT into account. However, an unexpected finding was made with regards to the balance between VAT and liver fat: in the presence of visceral obesity (high visceral fat), a balanced liver fat seemed to be important. Visceral obesity combined with high liver fat was strongly associated with T2D, while visceral obesity combined with a low liver fat was strongly associated with CVD.
This first evidence that differences in fat distribution patterns are not only associated with differences in magnitude of cardiometabolic risk, but also to differences in cardiometabolic risk profile (some patterns being more associated with T2D and others more with CVD), was followed up by a study illustrating the heterogeneity within obesity and metabolic dysfunctionassociated steatotic liver disease (MASLD)4. These findings were later validated prospectively in a study that combined data from the UK Biobank and Dallas Heart Study (DHS)5. The study included more than 22,000 UK Biobank participants (mean age 64 years and BMI 25.7 kg/m2, predominantly White [97%], followed for up to 5 years) and just above 2,000 Dallas Heart Study participants (mean age 44 and BMI 29.1 kg/m2, multi-ethnic cohort [32% White, 47% Black, 18% Hispanic], followed for up to 12 years).
Excluding participants with CVD and T2D at baseline, it investigated future risk of disease based on combinations of VAT and liver fat by partitioning people into categories of low–low, low–high, high–low, and high–high. The results showed it was more common to store your fat in a balanced way (the largest groups being the low–low [35.8%] and the high–high [35.9%]) than in a discordant way.
However, the group with visceral obesity and low liver fat (i.e., low–high), which was of primary interest for the investigation on future CVD events, was still fairly large (14.2%). Converging results across both the UK Biobank and Dallas Heart Study cohorts show that:
- For T2D, although high VAT was most strongly associated, both high VAT and liver fat significantly increased the risk of developing T2D, with the highest risk being observed for the high–high group:
- Unadjusted odds ratios (95% CI): 8.22 (5.59-14.72) and 7.81 (3.8515.85) for UK Biobank and Dallas Heart Study respectively
- Sex, age, and BMI adjusted odds ratios (95% CI): 3.68 (1.93-7.02) and 6.25 (2.86-13.67) for UK Biobank and Dallas Heart Study respectively
- For CVD, VAT was most effective in separating higher and lower risk individuals, with the highest risk being observed for the high–low group:
- Unadjusted hazard ratios (95% CI): 2.00 (1.65-2.43) and 2.42 (1.41-4.13) for UK Biobank and Dallas Heart Study respectively
- Sex, age, and BMI adjusted hazard ratios (95% CI): 1.50 (1.22-1.85) and 1.53 (0.86-2.71) for UK Biobank and Dallas Heart Study respectively
These results highlight that different individuals have different fat distribution patterns, which are in turn linked to various cardiometabolic disease risk profiles that may respond differently to treatments.
The results raise the question of whether or not drugs targeting reduction of liver fat should be evaluated for VAT reduction, to ensure significant lowering of the patients’ cardiometabolic risk. This is especially important, as results indicate lowering liver fat in people with a high VAT without resolving their visceral obesity may, in fact, put the patient at greater risk for heart disease.
2. AMRA® Researcher and fat distribution assessment in studies of incretin-based treatments
To date, there are four relevant studies with public results from fat distribution assessment using AMRA® Researcher that provide the first reference for treatments under development in the metabolic and weight management space:
Study 1
A randomised, double-blind, placebo-controlled, phase 4, single centre, 40 weeks trial of liraglutide (LIRA) 3.0 mg + lifestyle intervention vs placebo (PBO) + lifestyle intervention (NCT03038620)6:
- Including n=123 community-dwelling adults, BMI ≥ 30 kg/m² or BMI ≥ 27 kg/m² with metabolic syndrome but without T2D
- Primary endpoint: Percentage reduction in MRI VAT comparing LIRA to PBO
Study 2
A substudy of the randomised, open-label, parallelgroup, phase 3 SURPASS-3, multi-site (n=45 sites), 52 weeks trial of tirzepatide (TZP) 5, 10, 15 mg and insulin degludec (IDeg) (NCT03882970)7,8:
- Including n=296 adults with T2D, BMI ≥ 25 kg/m², stable weight, insulin-naive, on treatment w/ metformin +/- SGLT-2i, and FLI ≥ 60
- Primary endpoint: Absolute change in MRI liver PDFF comparing tirzepatide 10, 15 mg pooled to IDeg
Study 3
A substudy of the randomised, double-blind, placebo controlled, phase 2, multi-site, 48 weeks trial of retatrutide (RETA) 1, 4, 8, 12 mg vs PBO (NCT04881760)9:
- Including n=98 adults with BMI ≥ 30 kg /m2, or 27 ≤ BMI <30 kg/m2 with weight-related complications but without diabetes, liver PDFF ≥ 10%
- Primary endpoint: Mean relative change from baseline in MRI liver PDFF at 24 weeks comparing
all doses of RETA to PBO
Study 4
A prospective, single-site, 24 weeks, pilot study evaluating changes in MRI pancreatic PDFF following weight loss surgery (WLS)10:
- Including n=9 patients with severe obesity undergoing a weight-loss surgery program without history of known liver disease other than MASLD
All trials showed significant weight reduction ranging from 6.59% for 40 weeks of treatment with liraglutide combined with a lifestyle intervention, to 25.9% for 48 weeks of treatment with retatrutide. In addition to body weight reduction, participants also showed significant reduction of visceral, subcutaneous, and liver fat.

3. Introducing AMRA® Body Fat Z-Scores: Methodology, disease associations, risk-stratification, and effect from incretin-based treatments
Although more detailed descriptions of obesity and adiposity are important for achieving a deeper understanding of metabolic diseases, the collection of a wide range of measurements for a clinical trial naturally leads to challenges with trial design and endpoint usage/interpretation. The body fat Z-Scores indicate whether the patients’ underlying values (VAT, aSAT, or liver fat) are high, low, or as expected given their sex and BMI, which provide a reference within the biomarker itself. When used longitudinally, a zero change in Z-Score means the change in, e.g., VAT was in line with the weight change, whereas a significant reduction would mean the loss of VAT was larger than what can be described by the weight change – possibly indicating a targeted effect on VAT.
A body fat Z-Score is calculated by comparing each patient’s value to those of matched virtual controls and indicates how much they deviate (in standard deviations) from what is expected given their sex and BMI. Although the UK Biobank does not capture the wide variability of the world’s general population such as wider age ranges, ethnic representations, and diseases, the use of the same reference enables a robust comparison between every study participant in every clinical trial.
AMRA’s Z-Score methodology and its associations with future disease (CVD and T2D) was first published in The Journal of Clinical Endocrinology & Metabolism in 2023.11 Then, using the Z-Scores to investigate risk stratification within obesity class I & II (BMI 30-40 kg/m2) in 2024 showed that current guidelines for bariatric surgery based on BMI exclude some high-risk patients, which can be remedied by using the Z-Score methodology. The results were published in the American Surgery for Metabolic and Bariatric Surgery (ASMBS) guidelines/statements section of Surgery for Obesity and Related Diseases and showed that a high VAT Z-Score was associated with an increased risk for both CVD and T2D12.

Interestingly, the group with obesity class I & II and high VAT Z-Score had a higher risk for CVD than those with obesity class III indicating that there is a subset of patients with obesity class I that should be prioritized for targeted obesity treatment.
Later the same year, the Z-Scores were used to evaluate the effect on fat distribution pattern from tirzepatide treatment in the SURPASS-3 MRI study13. The study is the first to assess shifts in fat distribution in response to pharmacological treatment using weight-invariant body fat Z-Scores. The results showed a significant decrease in both VAT and liver fat Z-Scores, suggesting a potential targeted effect on VAT and liver fat. Overall, all Z-Scores moved towards zero, resulting in a shift towards a more balanced fat distribution pattern following treatment with tirzepatide.
Impact on the design and execution of future studies for obesity and metabolic diseases
AMRA’s concept for fat distribution assessment in clinical trials, including rapid and standardized image acquisition protocols, image processing, quality control procedures, as well as the unique body fat Z-Scores, has been developed specifically with outcomes and multi-site feasibility in mind.The large heterogeneity within obesity and metabolic diseases and the rapid development of a wide range of pharmacological treatments that achieve varying degrees of weight reduction pose a challenge in the clinical trial setting. Solving this challenge requires a scalable solution that can be implemented all the way from small Phase I studies to large Phase III & outcome trials, while providing clinically meaningful biomarkers that uncover effects beyond – and independent of – weight loss for treatment differentiation.
Absolute or percent changes in body weight and/or BMI are still typical endpoints in clinical trials evaluating treatments for obesity and related disorders. However, the body of evidence illustrating the clinical importance of more detailed descriptions of fat distribution patterns, coupled with the results from SURPASS-3 MRI, clearly illustrates that pharmacological treatments for T2D can alter the fat distribution pattern in various ways independent of weight change. This makes weight-invariant fat distribution assessment an attractive and modifiable endpoint for future trials in obesity therapeutic development.
References
- Neeland IJ, Ross R, Després J-P, Matsuzawa Y, Yamashita S, Shai I, Seidell J, Magni P, Santos RD, Arsenault B, et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: a position statement. The Lancet Diabetes & Endocrinology. 2019;7:715-725. doi: 10.1016/s2213- 8587(19)30084-1
- Borga M, Ahlgren A, Romu T, Widholm P, Dahlqvist Leinhard O, West J. Reproducibility and repeatability of MRI-based body composition analysis. Magn Reson Med. 2020;84:3146-3156. doi: 10.1002/ mrm.28360
- Linge J, Borga M, West J, Tuthill T, Miller MR, Dumitriu A, Thomas EL, Romu T, Tunon P, Bell JD, et al. Body Composition Profiling in the UK Biobank Imaging Study. Obesity (Silver Spring). 2018;26:17851795. doi: 10.1002/oby.22210
- Linge J, Whitcher B, Borga M, Dahlqvist Leinhard O. Sub-phenotyping Metabolic Disorders Using Body Composition: An Individualized, Nonparametric Approach Utilizing Large Data Sets. Obesity (Silver Spring). 2019;27:1190-1199. doi: 10.1002/ oby.22510
- Tejani S, McCoy C, Ayers CR, Powell-Wiley TM, Despres JP, Linge J, Leinhard OD, Petersson M, Borga M, Neeland IJ. Cardiometabolic Health Outcomes Associated With Discordant Visceral and Liver Fat Phenotypes: Insights From the Dallas Heart Study and UK Biobank. Mayo Clin Proc. 2022;97:225-237. doi: 10.1016/j.mayocp.2021.08.021
- Neeland IJ, Marso SP, Ayers CR, Lewis B, Oslica R, Francis W, Rodder S, Pandey A, Joshi PH. Effects of liraglutide on visceral and ectopic fat in adults with overweight and obesity at high cardiovascular risk: a randomised, double-blind, placebo- controlled, clinical trial. The Lancet Diabetes & Endocrinology. 2021;9:595-605. doi: 10.1016/ s2213-8587(21)00179-0
- Gastaldelli A, Cusi K, Fernández Landó L, Bray R, Brouwers B, Rodríguez Á. Effect of tirzepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI): a substudy of the randomised, open-label, parallel-group, phase 3 SURPASS-3 trial. The Lancet Diabetes & Endocrinology. 2022;10:393-406. doi: 10.1016/s2213- 8587(22)00070-5
- Cusi Kenneth. The effects of tirzepatide on liver fat content and abdominal adipose tissue in patients with type 2 diabetes (SURPASS-3 MRI). 57th Annual Meeting of the European Association for the Study of Diabetes; Virtual.
- Sanyal AJ, Kaplan LM, Frias JP, Brouwers B, Wu Q, Thomas MK, Harris C, Schloot NC, Du Y, Mather KJ, et al. Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: a randomized phase 2a trial. Nat Med. 2024;30:2037-2048. doi: 10.1038/s41591-024- 03018-2
- Covarrubias Y, Fowler KJ, Mamidipalli A, Hamilton G, Wolfson T, Leinhard OD, Jacobsen G, Horgan S, Schwimmer JB, Reeder SB, et al. Pilot study on longitudinal change in pancreatic proton density fat fraction during a weight-loss surgery program in adults with obesity. J Magn Reson Imaging. 2019;50:1092-1102. doi: 10.1002/jmri.26671
- Linge J, Cariou B, Neeland IJ, Petersson M, Rodriguez A, Dahlqvist Leinhard O. Skewness in body fat distribution pattern links to specific cardiometabolic disease risk profiles. J Clin Endocrinol Metab. 2024;109:783-791. doi: 10.1210/clinem/dgad570
- Linge J, Widholm P, Nilsson D, Kugelberg A, Olbers T, Dahlqvist Leinhard O. Risk stratification using magnetic resonance imaging-derived, personalized z-scores of visceral adipose tissue, subcutaneous adipose tissue, and liver fat in persons with obesity. Surg Obes Relat Dis. 2024;20:419-424. doi: 10.1016/j.soard.2024.01.009
- Cariou B, Linge J, Neeland IJ, Dahlqvist Leinhard O, Petersson M, Fernández Landó L, Bray R, Rodríguez Á. Effect of tirzepatide on body fat distribution pattern in people with type 2 diabetes. Diabetes Obes Metab. 2024;26:2446-2455. doi: 10.1111/dom.15566