
AMRA® Muscle & Function Composite Scores
Translating muscle composition heterogeneity into robust clinical trial endpoints
There is an urgent unmet need for biomarker solutions that provide robust clinical trial endpoints for evaluating severity and progression in neuromuscular diseases (NMDs).
The slow disease progression and highly heterogeneous nature of these disorders pose a specific challenge to the development of desperately needed treatments by complicating conduction of therapeutic clinical trials1. Traditionally, tests of functional performance (such as muscle strength or timed walking tests) have been used for tracking of natural progression and treatment evaluation. However, during the relatively short time span of a clinical trial, it has been difficult to detect significant changes.
The slow progression rate and compensatory response of the study participants (making robust detection unlikely), in combination with the high variability of the tests used (caused by, e.g., patient fitness/motivation and difficulties with standardization) have raised concerns about whether these tests are appropriate to use as endpoints for evaluation of treatment response in NMD1.
As the loss of function in NMDs is preceded by a continuous loss of muscle tissue coupled with accumulation of muscle fat, monitoring muscle composition has long been of interest and magnetic resonance imaging (MRI) has been extensively used to capture these changes. There are several reasons why muscle MRI could be an ideal candidate as a potential efficacy and surrogate endpoint in NMD therapeutic trials:
- Muscle has an inherent close relationship with the underlying disease and is the target organ of treatment within NMD,
- The high precision achievable through MRI makes it possible to detect significant changes within the duration of a clinical trial,
- There is significant evidence demonstrating that muscle fat content correlates with clinical outcomes in NMD, and
- Several studies have even observed changes in muscle fat content preceding changes in function within NMD.
These points illustrate that muscle MRI can be used to generate objective, low-variability data on muscle composition, suitable for defining clinical trial endpoints. However, while these properties are critical from an endpoint perspective, it is still not enough to effectively capture disease severity and progression in NMD clinical trials. Although all NMDs share the characteristic of continuous muscle tissue loss and accumulation in muscle fat that leads to loss of function, there is a large heterogeneity in muscle involvement both between individuals with the same disorder, as well as in disease activity between different muscles within the same individual.
Awareness of this challenge is currently pushing the field away from single-slice assessments and focusing on one muscle group alone, to volumetric assessment of many muscles and muscle groups throughout the whole body. However, choosing which muscles to characterize and follow when designing a clinical trial is important and will depend on the context of use. Two important factors to consider are that (1) different activities of everyday life depend on the functionality of different sets of muscles, and (2) despite rapid disease progression, some muscles may show little to no change during a clinical trial (i.e., normal appearing and end-stage muscles with little to no disease activity) and following them will drastically reduce the responsiveness of the biomarker.
To address these issues, AMRA has developed composite muscle biomarkers using whole-body MRI. These composite scores are calculated following strategic selection of muscles based on either the clinical outcome investigated (functional cross-sectional composite scores) or the specific disease pattern of each individual (whole-body longitudinal composite scores). The selection focuses the composite scores on the most relevant muscles for the context of use and reduces the variability of the measurement, thus enabling detection of subtle changes over time.
AMRA further supports NMD studies in large, multi-site clinical trials. Our expertise is built upon a foundation of established research efforts that have enabled multiple trials to address variability, including standardized and efficient (30–45 min) scanning protocols, image calibration and segmentation, as well as robust quality control procedures.
Here, we present highlights from AMRA’s recent support in NMD therapeutic trials, including standardized scanning protocols, image processing, quality control procedures, and MRI-based composite muscle biomarkers. Multiple clinical trials leverage AMRA’s musculoskeletal quantification and scientific expertise to generate objective evidence to support data-driven decisions, notably in research on facioscapulohumeral muscular dystrophy (FSHD), Duchenne muscular dystrophy (DMD), and sporadic inclusion body myositis (sIBM).
Development and validation of MRI-based biomarkers and composite scores in FSHD
Together, the results from initial studies on facioscapulohumeral muscular dystrophy (FSHD), which were conducted in collaboration with Fulcrum Therapeutics, demonstrated the feasibility of implementing whole-body MRI in a multi-site clinical trial setting, as well as the value of using MRI based composite biomarkers as endpoints in FSHD (Figure 1). Standardized image acquisition protocol and post-processing methods were developed and validated with high performance (as published in Muscle & Nerve2), and the composite biomarkers were found to accurately capture disease severity and track disease progression while considering the highly heterogeneous nature of FSHD. This resulted in these being used as secondary endpoints in Fulcrum’s phase 2b trial ReDUX4 (NCT04003974) as well as in the large, multi-site phase 3 study REACH (NCT05397470) (as published in Neurology3 and Lancet Neurology4).
Seventeen adult participants with FSHD1, clinical severity score 2 to 4 (Ricci’s scale, range 0–5), were enrolled across 6 study sites and imaged twice, 4 to 12 weeks apart. Follow-up scans were carried out on 16 patients 52 days (range 36–85 days) later. Thirty-six muscles (18 bilaterally) from shoulder, arm, trunk and legs were segmented volumetrically using a semi-automated multi-atlas-based segmentation, with muscle fat fraction (MFF), muscle fat infiltration (MFI) and lean muscle volume (LMV) quantified.
For technical validation, repeatability of MFF, MFI and LMV was assessed both for all individual muscles as well as for the muscles combined. Within patient standard deviation (SD) ranged from 1.00% to 3.51% for MFF and 0.40% to 1.48% for MFI across individual muscles. When all muscles were combined, the SDs were improved (0.70% and 0.32% for MFF and

Figure 1 Overview of AMRA® Muscle & Function Composite Scores. The figure illustrates the musculoskeletal quantification biomarkers suited for neuromuscular disease trials supported by AMRA: lean muscle volume (LMV), muscle fat fraction (MFF), and muscle fat infiltration (MFI). Muscles are categorized as A, B, or C, and these measures are integrated into whole-body longitudinal and functional composite scores. The latter utilize region-specific muscle groupings relevant to clinical outcome assessments, such as the Timed Up and Go (TUG) and Reachable Workspace (RWS) tests.
MFI respectively). For LMV, coefficients of variation ranged from 2.7% to 11.7% across individual muscles and reached as low as 2.0% when all muscles were combined. The results clearly illustrate that measurement performance can be drastically improved through volumetric assessment of multiple muscles throughout the body.
For clinical validation, the functional cross-sectional composite scores were associated with standard clinical outcome assessments (timed up and go [TUG], FSHD-TUG, and reachable workspace [RWS]) demonstrating moderate to strong correlation of MFF and MFI with TUG (ρ = 0.71 and ρ =0.83; Figure 2), FSHD-TUG (ρ = 0.73 and ρ = 0.73) and RWS (left arm: ρ = −0.71 and ρ = −0.53; right arm: ρ = −0.61 and ρ = −0.65). The whole-body longitudinal composite score, calculated following the strategic selection of muscles categorized as intermediate B muscles (high risk of progression compared to normal A muscles or end-stage C muscles) at baseline, was shown to capture the disease heterogeneity of FSHD while serving as a robust measure to track longitudinal changes in therapeutic clinical trials.
The phase 2b trial ReDUX4 enrolled 80 adults aged 18-65 with FSHD1, Ricci clinical severity score of 2–4, and at least one skeletal muscle judged using MRI to be suitable for biopsy (40 randomized to losmapimod and 40 to placebo) across 17 neurology centers in Canada, France, Spain, and the USA. The study concluded that although losmapimod did not significantly change DUX4-driven gene expression (primary endpoint), it was associated with potential improvements in prespecified structural outcomes (muscle fat infiltration; mean [95% CI ] treatment difference -0.49 [-0.86 to -0.12] percentage points, p = 0.010), functional outcomes (RWS), and patient-reported global impression of change compared with placebo. The findings informed the design and choice of efficacy endpoints for the phase 3 REACH trial, which ultimately enrolled 260 patients across 33 sites with RWS as primary endpoint and MFI, shoulder adductor strength, Patient Global Impression of Change (PGIC), and the Neuro QoL Upper Extremity as secondary endpoints.

Figure 2a The leg muscles functional composites of MFF and MFI correlate with the functional Timed Up and Go (TUG) test in individuals with FSHD. Adapted from Mellion ML, et al., 20223.
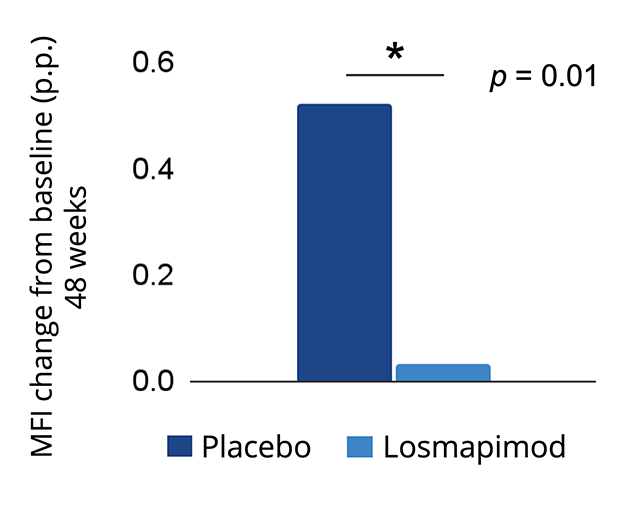
Figure 2b The B-muscles longitudinal composite revealed thatlosmapimod treatment resulted in a smaller increase in MFI from baseline compared to placebo in the ReDUX4 FSHD clinical trial. Adapted from Tawil R, et al., 20244.
MRI muscle measurements correlate strongly with functional changes and were shown to precede changes in functional performance within a DMD clinical trial
Generalizability of AMRA’s MRI-based quantitative biomarkers has been demonstrated by moving the concept from a slowly progressing, highly heterogeneous NMD (FSHD) to a rapidly progressing, homogeneous NMD (Duchenne muscular dystrophy [DMD]). The post-hoc analysis of Pfizer’s clinical study (NCT02310763) of domagrozumab (an antibody targeting myostatin that negatively regulates skeletal muscle mass) published in Muscle & Nerve5, further illustrated the relevance of MRI muscle measurements in correlating with functional changes. The study showed clearassociations between muscle compositional changes and functional performance tests used as clinical outcome assessments in DMD.
Importantly, changes in MRI measurements were shown to precede changes in functional performance, suggesting their superior sensitivity for tracking disease activity and supporting their use as potential surrogate endpoints in therapeutic clinical trials. Similar to what was observed in FSHD with regard to rate of progression in muscles characterized as intermediate B muscles compared to normal A muscles or late-stage C muscles, results indicated that muscles with moderately increased fat content at baseline showed faster progression compared to those with low or very high fat content, motivating the usefulness of implementing the whole-body longitudinal composite score based on baseline muscle categorization alsoin DMD.
Ninety-eight boys with DMD assessed at baseline, and week 17, 33, 49, and 97 were included for progression analysis. Images covering a single thigh from the hip to the knee were previously acquired and the adductors, hamstrings and quadriceps muscles were segmented volumetrically using a semi-automated multi-atlas-based segmentation for quantification of muscle fat fraction (MFF), muscle fat infiltration (MFI), and lean muscle volume (LMV). The post-hoc analysis focused on associations of change from baseline (78 patients with available MRI data), to week 49 (67 patients with available MRI data), and week 97 (33 patients with available MRI data) in MFF, MFI, and LMV with change in the North Star Ambulatory Assessment (NSAA; a validated clinical outcome assessment test for the evaluation of functional motor abilities in ambulant children with DMD).
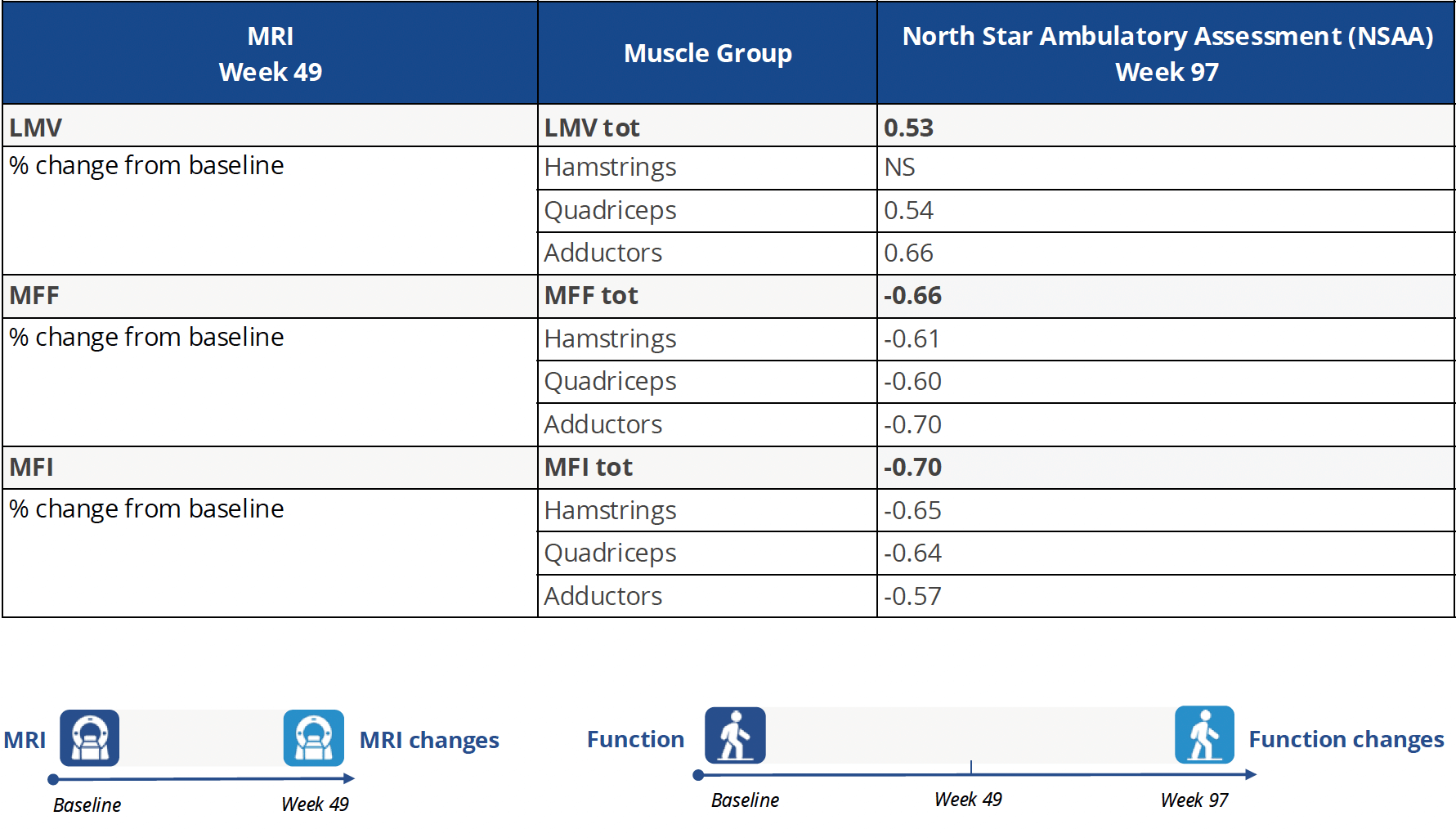
The study added to the clinical validation of AMRA’s MRI biomarkers by showing correlation with functional performance: Low MFF & MFI values and high LMV values (indicating normal muscle composition) coincided with high NSAA scores (indicating good functional performance) with significant cross-sectional correlations for MFF (ρ = -0.61, p < 0.001), MFI (ρ = -0.64, p < 0.001), and LMV (ρ = 0.51, p < 0.001). In addition, changes in MRI biomarkers at week 49 were significantly correlated with changes in NSAA at week 97 (MFF: ρ = -0.66, MFI: ρ = -0.70, LMV: ρ = 0.53, all p < 0.001), Figure 3.
Figure 3 MRI change from baseline to week 49 correlates with functional change at week 97 (North Star Ambulatory Assessment) in participants of a DMD clinical trial. The data show that MRI changes precede changes in functional performance. Adapted from Sherlock SP, et al., 20245.
Confirming the utility of MRI-based muscle measurements in sporadic inclusion body myositis (sIBM)
Widened generalization of AMRA’s MRI-based quantitative biomarkers has been illustrated by moving the concept beyond FSHD and DMD into inflammatory myopathies through application in inclusion body myositis (sIBM). The study, performed in collaboration with the National Center of Neurology and Psychiatry in Tokyo and Japanese pharmaceutical company Daiichi-Sankyo, and published in Muscle & Nerve6, showed high repeatability of MRI biomarkers and illustrated clinical relevance through strong correlations with tests of functional performance commonly used as endpoints in sIBM clinical trials. Like with FSHD and DMD, the study showed that muscles categorized as intermediate B muscles at baseline had a faster progression rate compared to those categorized as normal A muscles, further illustrating the strength in generalization of AMRA’s whole-body longitudinal composite scores for NMD clinical trials across various indications.
Ten sIBM patients were scanned at baseline and at 12 months, acquiring images that covered the entire leg. The individual muscles, which included the quadriceps, hamstrings, adductors, gastrocnemius and tibialis anterior muscles, were segmented volumetrically using a semi-automated multi-atlas-based segmentation for quantification of muscle fat fraction (MFF), muscle fat infiltration (MFI), and lean muscle volume (LMV).
Baseline test-retest MRI measurements were used to estimate within-subject variation and repeatability. Assessment of functional performance included knee extension strength tests and inclusion body myositis-functional rating scores (‘Total IBMFRS’ and ‘IBMFRS-LL’ specific to lower limb).
The results showed high reproducibility of repeat scans, with better performance for the larger muscle groups in the thighs (compared to the smaller muscles in the lower leg) and for muscles categorized as normal (A) or intermediate (B) (compared to end-stage C muscles) at baseline, Figure 4a. Correlations of MFF, MFI, and LMV with knee extension, ‘Total IBMFRS’ and ‘IBMFRS-LL’ were all significant with the strongest correlations observed when matching the muscle-specific knee extension strength test with quadriceps measurements (Figure 4b, LMV: ρ = 0.97, MFF: ρ = -0.90, MFI: ρ = -0.90, all p < 0.001) and the more general ‘Total IBMFRS’ functional performance test with MFF and MFI measurements combining all muscles (MFF: ρ = -0.91, MFI: ρ = -0.96, both p < 0.001).

Figure 4a Longitudinal changes in MFI, MFF, and LMV composite scores show that B muscles progress faster than A muscles in sIBM participants over 12 months. Adapted from Heerfordt J, et al., 20246.
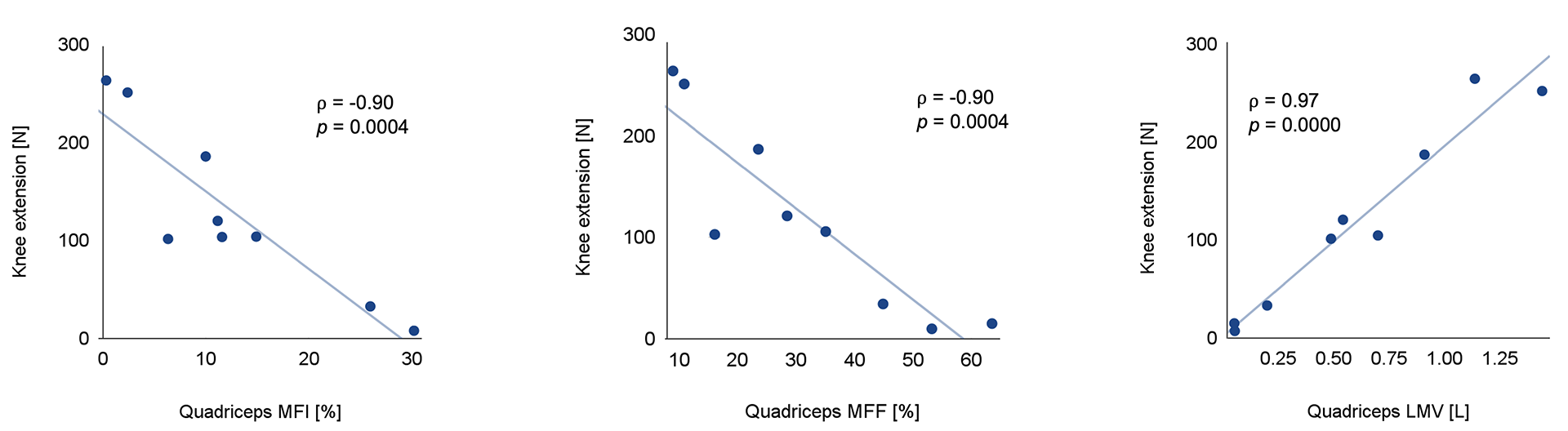
Figure 4b Baseline quadriceps MRI biomarkers strongly correlate with knee extension strength in sIBM participants. Adapted from Heerfordt J, et al., 20246.
Impact on the design and execution of future studies for neuromuscular diseases
The heterogeneous nature and slow progression of NMDs, combined with their rarity, pose a specific challenge in the clinical trial setting. These challenges require clinically meaningful study endpoints (linked to the disease process and how the participants feel and function) with very high technical performance enabling studies with fewer patients and shorter durations relative to the rate of disease progression.
AMRA facilitates NMD research by providing musculoskeletal measurements and scientific insights to support the advancement of clinical trials. This capability is built upon a robust foundation of proprietary research and data acquired from multiple studies across several NMDs. The framework developed for NMD therapeutic trials is grounded in extensive scientific investigations that have shaped the standardized scanning protocols, image processing and quality control procedures, as well as the unique functional cross-sectional and whole-body longitudinal composite scores. This approach enables AMRA to support clinical trials specifically with a study endpoint perspective and multi-site feasibility in mind.
This first wave of studies clearly illustrates AMRA’s drive and deep commitment to strengthening our knowledge of NMDs and supporting the development of desperately needed therapies. The composite biomarkers have gone through methodological qualification and rigorous scientific assessment, indicating their promise as future efficacy and surrogate endpoints in NMD clinical trials. Following the initial development, done in collaboration between AMRA and Fulcrum, the concept has proven scalable across Fulcrum’s complete development program for FSHD (a slow progressing, heterogeneous NMD), which has utilized the composite biomarkers as pre-defined endpoints. Published results from DMD (a rapidly progressing, homogeneous NMD) and sIBM (an inflammatory myopathy) indicate high generalizability of the framework and the potential of AMRA’s concept for NMD to revolutionize the clinical trial landscape across a wide range of indications.
References
- Dahlqvist JR, Widholm P, Leinhard OD, Vissing J. MRI in Neuromuscular Diseases: An Emerging Diagnostic Tool and Biomarker for Prognosis and Efficacy. Annals of Neurology. 2020;88:669-681. doi: 10.1002/ana.25804
- Widholm P, Ahlgren A, Karlsson M, Romu T, Tawil R, Wagner KR, Statland JM, Wang LH, Shieh PB, van Engelen BGM, et al. Quantitative muscle analysis in facioscapulohumeral muscular dystrophy using whole-body fat-referenced MRI: Protocol development, multicenter feasibility, and repeatability. Muscle Nerve. 2022;66:183-192. doi: 10.1002/mus.27638
- Mellion ML, Widholm P, Karlsson M, Ahlgren A, Tawil R, Wagner KR, Statland JM, Wang L, Shieh PB, van Engelen BGM, et al. Quantitative Muscle Analysis in FSHD Using Whole-Body Fat-Referenced MRI: Composite Scores for Longitudinal and Cross-Sectional Analysis. Neurology. 2022;99:e877-e889. doi: 10.1212/ WNL.0000000000200757
- Tawil R, Wagner KR, Hamel JI, Leung DG, Statland JM, Wang LH, Genge A, Sacconi S, Lochmuller H, Reyes-Leiva D, et al. Safety and efficacy of losmapimod in facioscapulohumeral muscular dystrophy (ReDUX4): a randomised, double-blind, placebo- controlled phase 2b trial. Lancet Neurol. 2024;23:477-486. doi: 10.1016/ S1474-4422(24)00073-5
- Sherlock SP, McCrady A, Palmer J, Aghamolaey H, Ahlgren A, Widholm P, Dahlqvist Leinhard O, Karlsson M. Relationship Between Quantitative Magnetic Resonance Imaging Measures and Functional Changes in Patients With Duchenne Muscular Dystrophy. Muscle Nerve. 2024. doi: 10.1002/mus.28321
- Heerfordt J, Karlsson M, Kusama M, Ogata S, Mukasa R, Kiyosawa N, Sato N, Widholm P, Dahlqvist Leinhard O, Ahlgren A, et al. Volumetric muscle composition analysis in sporadic inclusion body myositis using fat‐referenced magnetic resonance imaging: Disease pattern, repeatability, and natural progression. Muscle & Nerve. 2024. doi: 10.1002/mus.28252